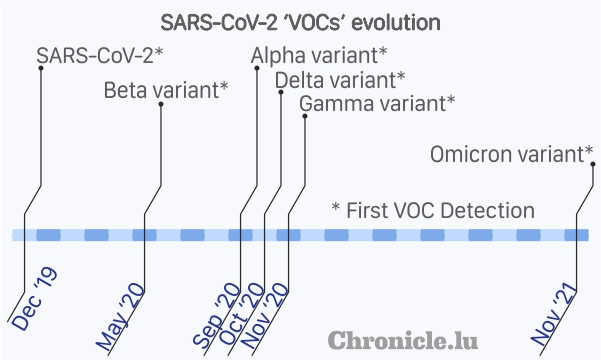
 SARS-CoV-2 Variants of Concern (VOC) evolution timeline;
Credit: Kangkan Halder
SARS-CoV-2 Variants of Concern (VOC) evolution timeline;
Credit: Kangkan Halder
What is the Omicron variant and why it is suddenly so important?
Omicron is a mutant of the original SARS-CoV-2 virus and the most divergent variant to date. It has between 26 and 32 mutations, three deletions and one insertion in the spike protein and has epidemiological consequences as the current RNA based vaccines are against the original spike protein genetic sequence. A large number of changes in the genetic sequence, like in the case of Omicron, would lead to a dramatically different spike protein shape and surface area. Hence, the antibodies generated by current generation RNA vaccines against the original sequence can no longer recognise this evolved spike protein of the Omicron variant. This is also known as "immune evasion" and is a major concern under the current ongoing pandemic.
Why is the mutant called Omicron?
According to the Phylogenetic Assignment of Named Global Outbreak LINeages (Pangolin) nomenclature, the variant was originally named as B.1.1.529 lineage.
The Technical Advisory Group on SARS-CoV-2 Virus Evolution at the World Health Organization (WHO), a specialised group which renames the lineages according to Greek alphabets in terms of Variant of Interest (VOI) and Variant of Concern (VOC) which in turn depends on the severity of transmissibility and virulence of the variant.
The B.1.1.529 variant from South Africa was first reported to WHO on 24 November 2021 and the first known confirmed B.1.1.529 infection was from a specimen collected on 8 November 2021.
Based on the initial data and a rapid increase in cases in South Africa, WHO designated the B.1.1.529 lineage as a VOC and named it Omicron on 26 November 2021.
How quickly is Omicron spreading?
The weekly report for 21 to 27 November 2021 from the National Institute for Communicable Diseases (NICD), a division of the National Health Laboratory Service (NHLS) in South Africa reported 13,656 new cases, a stellar 241.6% increase from a week before.
Of these 13,656 cases detected, 10,821 (79.2%) were from the Gauteng province, the same province from which the first Omicron sample was collected on 8 November 2021 and sequenced. In the past three weeks, over 200 samples were sequenced from the Gauteng province and 90% of them were of Omicron lineage. Nationally, Omicron prevalence was 73% for the month of November 2021 in South Africa (a total of 312 samples sequenced).
Together, these initial data show a remarkable increase in cases, especially the Omicron variant in South Africa.
Does Omicron result in any different symptom(s) compared to other variants?
According to the NICD in South Africa, currently there are no unusual symptoms reported following infection with Omicron variant and some individuals are asymptomatic, as was the case with previous variants.
How many Omicron cases have been detected so far?
According to the European Centre for Disease Prevention and Control (ECDC), as of 6 December 2021 there were a total of 212 confirmed cases in the European Union (EU) and European Economic Area (EEA) and 905 confirmed cases globally reported by 47 countries.
Does Omicron have a higher virus transmissibility (infectiousness)?
There is not enough data yet and any preliminary estimations are likely to be revised. Therefore the following texts should be considered with caution and to be understood as "first estimations only".
According to Tom Wenseleers, Professor of biostatistics at the Katholieke Universiteit (KU) Leuven, Belgium, Omicron can infect up to six times as many people as the Delta variant, over the same time period.
Does Omicron evade vaccine-induced immunity?
Again, there is not yet enough data to conclusively confirm this. However, the initial hypothesis indicated that Omicron could evade natural (post-infection with other variants) as well as vaccine-induced immunity (see first question for explanation).
In South Africa, which has a vaccination rate of about 25% and according to a pre-print publication (1 December 2021) from the South African DSI-NRF Centre of Excellence in Epidemiological Modelling and Analysis team, the reinfection rate versus primary infection rate for the period from 1 November 2021 to 27 November 2021 in comparison to the first wave was 2.39 times, meaning the new cases in South Africa are 2.39 times more likely to be contracted by an individual who was infected before. Hence, Omicron seems to evade natural immunity.
Prof. Wenseleers further argued that the sudden rise in cases in South Africa are contributed by high transmissibility and immunity evasion and it is assumed for the time being that Omicron is less contagious than Delta. This means that the situation in South Africa can only be explained by immune evasion, and this will translate into up to five times more than the immune evasion seen in Delta.
Scientifically speaking, the effectiveness of a booster dose against the Omicron variant has not yet been assessed.
Does Omicron have a higher hospitalisations rate, death rate or disease severity?
Here again, there is not yet enough data to conclusively say anything and we need to wait for health agencies to collect and provide relevant data.
Does Omicron affect a certain age group?
An assessment of risk factors for certain age groups is relevant when there is a community transmission and all the population is at risk of infection. Currently, there are sparse data on community transmissions. In South Africa, the highest weekly incidence risk among cases detected between 21 to 27 November 2021 was reported in the 25-44 year age group for all variants together.
Epidemiologically, the older population with low immunity, immunocompromised people and people with co-morbidity remain at higher risk of adverse effect compared to the general population.
Is there any way to minimise the Omicron spread?
To limit the risk of contracting and spreading Omicron, as with any other variant, it is recommended to:
- get vaccinated against COVID-19 and get a booster dose when available;
- wear a face mask properly covering the nose and mouth;
- avoid unnecessary gatherings, especially those in closed spaces for longer durations;
- keep a social distance of one metre or more;
- wash hands regularly with soap and water.








