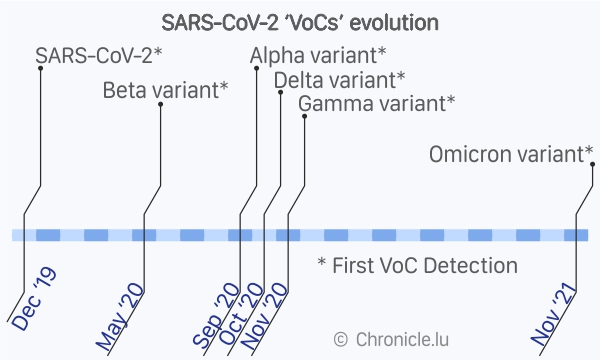
The Omicron variant of the SARS-CoV-2 virus, first reported by South Africa on 24 November 2021 to the World Health Organisation (WHO), is an exceptionally evolved variant: it has between 26 and 32 mutations, three deletions and one insertion in the spike protein, making it highly divergent from the original variant.
This also means, in epidemiological terms, that the number of reinfections would increase as the currently available mRNA-based COVID-19 vaccines are targeted against the original spike protein genetic sequence, which has low resemblance to the Omicron spike protein, and hence the vaccine-generated antibodies would not recognise effectively.
The Omicron VoC (variant of Concern) is also unique in terms of its transmissibility rate, estimated to be able to infect up to six times as many people as the Delta varaint over the same period of time, according to the Professor of biostatistics Tom Wenseleers at the Katholieke Universiteit (KU) Leuven, Belgium. Based on epidemiology data from South Africa, the United Kingdom, the European Union (EU) and European Economic Area (EEA) countries, Omicron became the dominant variant in less than four weeks in most settings, including Luxembourg.
Globally, in a recent three week period (10 to 30 January 2022) witnessed 20 million new cases every week, a four-fold increase compared to peaks of around 5 million weekly cases before November 2021, when Omicron was not present. At least 5.6 million deaths globally due to COVID-19 has been documented since the beginning of the pandemic.
However, even though the case notification rates (bi-weekly number of positive cases per 100,000 residents) in the EU/EEA was three times higher than the highest peak observed during the pandemic up to then, according to the European Centre for Disease Prevention and Control (ECDC) report dated 27 January 2022, hospitalisation rates and mortality rates remain below the levels observed in earlier pandemic waves, underlining mild symptomatic cases and reduced servere outcomes.
By the first week of 2022, Omicron was the most common variant in the EU/EEA.
In terms of symptoms, the National Institute for Communicable Diseases (NICD) in South Africa, where the first cases appeared, reported no unusual symptoms compared to earlier variants. The latest update from the (US) Center for Disease Control and Prevention (CDC) dated 2 February 2022 also noted Omicron symptoms similar to previous variants. The WHO, in its latest report dated 27 January 2022, referred to preliminary data from the United Kingdom, wherein Omicron infections appeared to be associated with more frequent sore throat than for Delta variant and reduced frequency in loss of smell and taste.
In other media reports, infectious disease consultant Dr Eoghan de Barra at Beaumont Hospital, Dublin, reported many people with Omicron have headaches, runny noses and low energy without chest pains or oxygen requirements from previous infections.
Further underscoring the unique features of Omicron, the ECDC has noted in research from Japan on Omicron viral shedding using 83 specimens taken from nineteen vaccinated people and two unvaccinated people, that levels of viral RNA were highest at three to six days from diagnosis or symptom onset and gradually decreased over time with no infectious virus (using virus culture) detected in the respiratory samples after ten days since symptoms onset - resulting in low detection rates of Omicron by PCR when people start having symptoms, especially for nasopharyngeal (NP) samples, but more often at three to six days from symptom onset. However, the average duration of PCR positivity remained at 9.87 days for Omicron compared to 10.9 days in case of Delta, meaning no adjustments in the isolation or quarantine period is needed at present.
In terms of viral replication, WHO noted research from Hong Kong University showing up to 70 times faster replication in the human bronchi (respiratory tract) compared to the Delta variant but relatively much slower replication in the lungs. The high replication rates might partially reason for the high transmissibility rates.
The ECDC clarified that there is no data so far on the incidence of prolonged symptoms after COVID-19 (long-COVID) due to Omicron.
Overall, there is lack in consensus amongst the scietific community on Omicron symptoms differing from the other variants and its clinical manifestations, other than Omicron infections presenting low severe outcome (hospitalisation and mortality) compared to previous waves.
Sources:
https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html
https://www.who.int/docs/default-source/coronaviruse/2022-01-21-global-technical-brief-and-priority-action-on-omicron-sars-cov-2-variant.pdf
https://www.ecdc.europa.eu/sites/default/files/documents/RRA-19-update-27-jan-2022.pdf







